 loading
loading
featuresBalancing ActFor people with diabetes, finding the equilibrium between sugar and insulin is a matter of survival—every day. Elizabeth Svoboda ’03, a California-based science writer, also contributes to Fast Company, Popular Science, and Discover.  Illustration by Alex NabaumView full image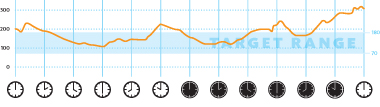 Mark Zurolo ’01MFAView full imagePizza = High Studies show that if people with diabetes can keep their blood-sugar levels within a target range (70 to 180 milligrams of glucose per deciliter of blood), they develop fewer complications from diabetes. But these graphs, which chart blood-sugar levels in a child over two 24-hour periods two days apart, show how hard it is to keep on target. In the first graph, blood sugar is relatively good until after bedtime, when it rises above 300. This pattern, says Stuart Weinzimer, is “a classic response to a pizza dinner.” Patients can program their pumps to deliver doses of insulin while they sleep, but the fats in pizza throw their calculations off by delaying the body’s absorption of carbohydrates for several hours. 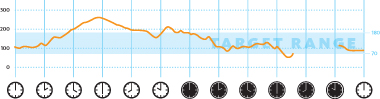 Mark Zurolo ’01MFAView full imageExercise = Low In the second graph, a morning high—perhaps due to insufficient insulin overnight—is followed by good numbers during the day and then low blood sugar in the evening and into the night. (Gaps like the one shown here occur when the sensor is not working properly.) Overnight lows, when a subject is asleep, are especially dangerous. This one is likely related to daytime exercise, which increases the body’s sensitivity to insulin. As with fatty foods, these effects are delayed, and their timing is unpredictable. With the artificial pancreas, the prolonged lows and highs would be reduced. The insulin pump would automatically deliver more insulin as sugar levels started to rise and suspend delivery to prevent lows. Ben Yarmis, 18 years old, is prostrate in a white-sheeted bed on the tenth floor of Yale–New Haven Hospital, hooked up to an IV and surrounded by doctors and technicians. You might assume he wishes he were outside on this glorious late-summer afternoon, but he’s thrilled to be just where he is right now. Yarmis, a George Washington University freshman who loves computer gaming and obscure rock bands, is participating in a trial of the first ambulatory automated insulin delivery system—a so-called artificial pancreas. Whenever a healthy person so much as glimpses food or smells it cooking, the pancreas starts to churn out insulin, a hormone that stimulates the body’s cells to take up ingested sugars from the bloodstream for their energy supply. But because of Yarmis’s type 1 diabetes, a condition he was diagnosed with at age 11, his pancreas no longer produces insulin reliably. He has to give himself multiple insulin doses daily and monitor his blood sugar to prevent it from creeping too high or too low—dangerous conditions that, at extreme levels, could cause delirium or a diabetic coma. If his blood sugar levels stray too often, even moderately, over the long term they could cause damage leading to heart disease, blindness, or loss of limbs. For the past seven years, Yarmis’s life has been punctuated with constant diabetes management. It’s not just a simple question of countering food with insulin. Blood sugar can go up or down dramatically and unpredictably because of an extra apple, a dash for the bus, a lost hour of sleep. Moreover, the body responds differently to insulin at different times of the day, and the liver can release glucose into the blood hours after a person has eaten. Slipups are inevitable. “I check my glucose number a lot,” Yarmis says, but “a lot of this is just controlling it by the seat of my pants.” This clinical trial run by Yarmis’s doctor, Yale endocrinologist Stuart Weinzimer ’88, has granted him a short reprieve from his blood-sugar management regimen. For three days, he will eat, sleep, and exercise for carefully timed periods under the watchful eyes of a team of doctors, nurses, and researchers, all while wearing two electronic devices that together might make up for his lack of a functioning pancreas. “This is the transmitter part that pops through his skin,” explains Weinzimer, pointing to a silver-dollar-sized gray circle taped to Yarmis’s abdomen. The sensor underneath continuously monitors his blood glucose levels and sends the data to a small blue computer on a belt clip, about the size of a Game Boy. “The transmitter beams data to this device,” Weinzimer says, “which signals the insulin pump.” Software developed by the manufacturer, Medtronic, directs an insulin reservoir to dispense doses appropriate for Yarmis’s current blood sugar levels. They enter his body via a narrow length of plastic tubing that feeds into a cannula inserted under his skin. Yarmis will wear the sensor and the pump throughout his three days in the hospital. Continuous glucose monitors (CGMs) and insulin pumps aren’t new. Many diabetics already use them for checking their blood sugar and dosing themselves with the sugar-lowering hormone. But the artificial pancreas Weinzimer is testing, developed by the Minneapolis-based Medtronic, closes the loop—making an electronic connection between the CGM and the insulin pump, so that the wearer doesn’t need to determine when to take insulin or how much. Many different companies are working on versions of an artificial pancreas; Medtronic’s is the first in clinical trial. Its software allows the CGM to feed blood glucose readings to the insulin pump, which reacts by administering the amount of insulin needed to keep sugar levels within a normal range. “It automates the process so you don’t have to make adjustments all the time,” Weinzimer says. That means wearers like Yarmis can—in theory, anyway—go on complete diabetes autopilot. Better yet, if the device works as it should, they’ll be able to live their lives free of the fear of debilitating complications as they age. Yarmis will remain hooked up to the artificial pancreas for about 72 hours straight. On the first day, he’ll have to stay quiet and still—“like a couch potato,” Weinzimer says. On the second day, things will start ramping up. For instance, he’ll run on a treadmill in the corner of the room for about an hour to make sure the “pancreas” adapts properly to the body’s insulin needs when he’s exercising. Yarmis knows malfunctions are a possibility, but when I ask him how he feels about that, he says he’s not nervous. More than anything, he says, “I feel lucky.”
|

|
 Print
Print Email
Email