 loading
loading
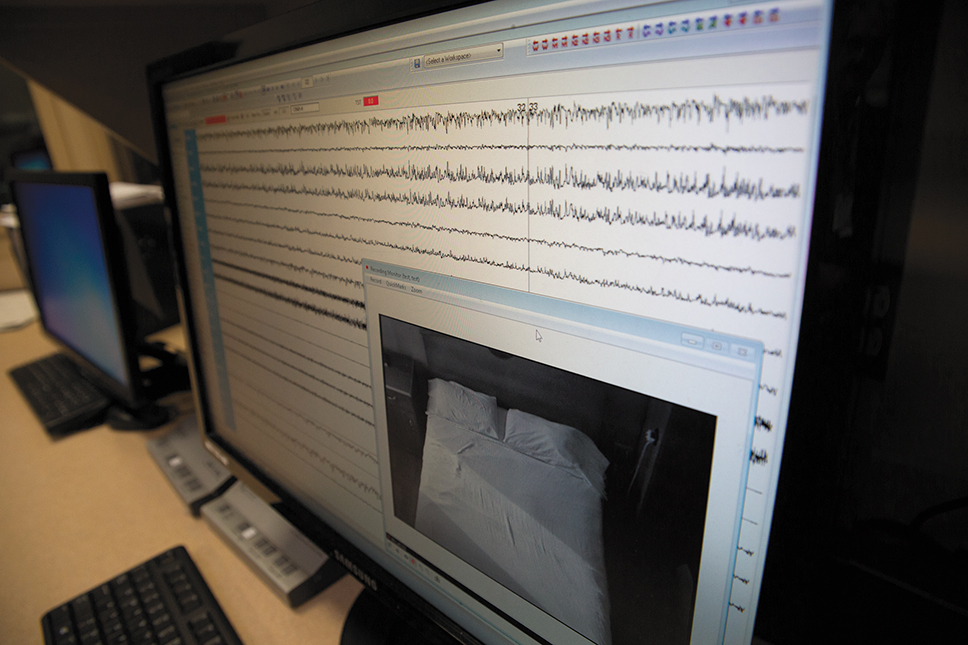
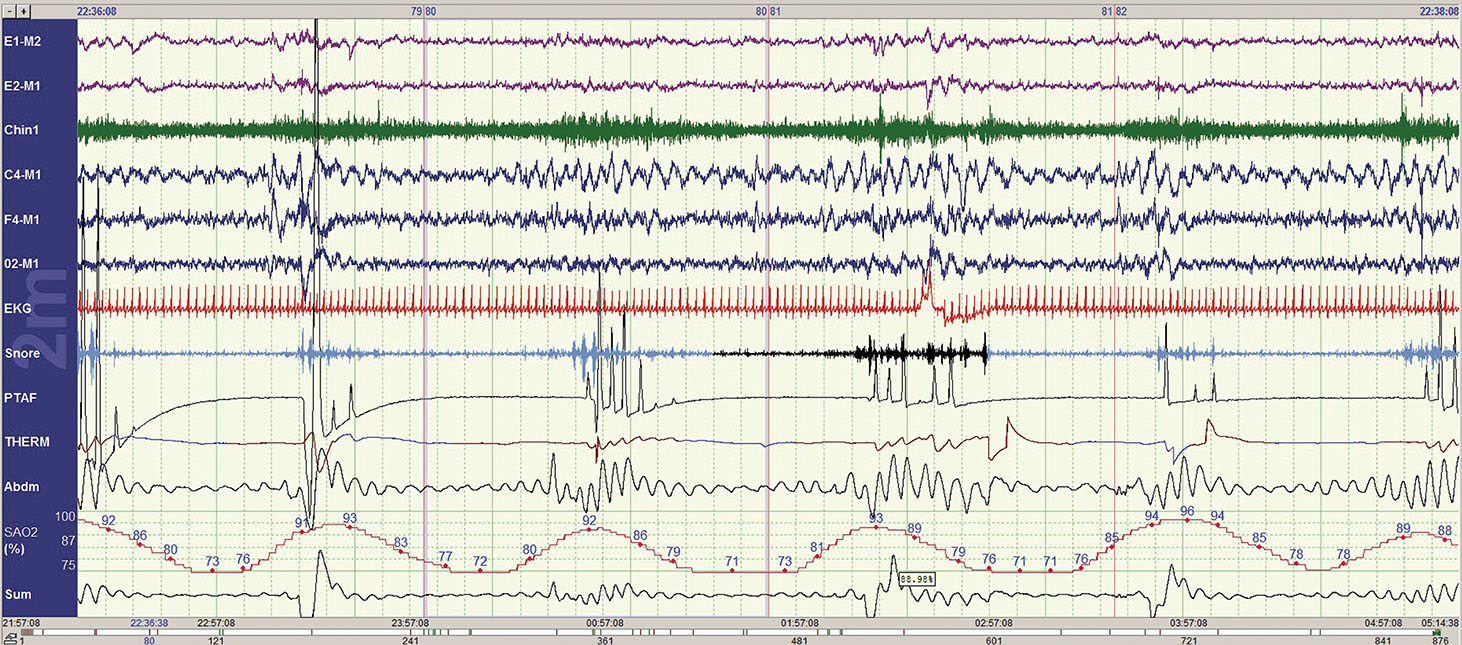
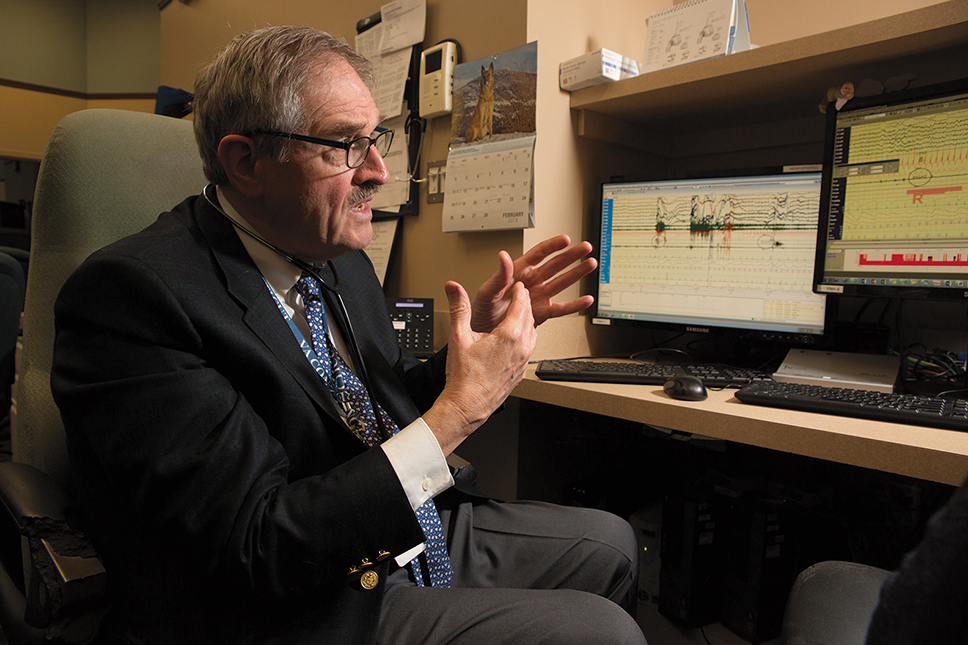
featuresTrouble sleeping? There’s hope.Meir Kryger has treated more than 30,000 people who have sleep problems. And it usually works. Tina Kelley ’85, coauthor of Almost Home: Helping Kids Move from Homelessness to Hope, is a writer at Covenant House. She was a New York Times reporter for ten years. Inside, at nighttime, the Yale New Haven Hospital’s Sleep Medicine Center in North Haven looks like a cross between a business-class hotel and an air traffic control center. A core of computers monitors up to a dozen sleepers—or would-be sleepers—at a time, recording breathing patterns, brain waves, heart rate, and other data. The patients who come here are the truly weary, referred here because their problems have not responded to regular treatment. Many have insomnia. Some have sleep apnea, the dangerous cessation of breathing during sleep due to an obstructed airway. Some have restless leg syndrome—a discomfort in the limbs that compels the sufferer to move for relief, disrupting sleep again and again. The science of sleep, a relatively new field, is being explored here by one of its earliest practitioners. As a medical resident at McGill University in 1973, Meir Kryger observed that a patient of his who had been admitted with seizures was struggling to breathe in his sleep. Kryger discovered that the man would stop breathing for up to a minute repeatedly during the night. When his struggles were at their worst, his heart would stop for nearly ten seconds, causing the seizures. Kryger’s journal article on the case was one of the first papers on sleep apnea in North America. Kryger, now a professor of medicine and clinical professor of nursing at the Yale School of Medicine, has made the study and treatment of sleep disorders his life’s work. When he started working in sleep medicine, the clinical field essentially didn’t exist. There were no courses to take, no books to study, and no sleep clinics; in North America, there was one lab at Stanford that studied patients clinically, and it focused mainly on narcolepsy. Kryger learned directly from his patients. Today, he is chief editor of the leading textbook in the field—The Principles and Practice of Sleep Medicine—and has won numerous awards for his work. Among other breakthroughs, he published the first research using computers to analyze breathing patterns during sleep, and research at his lab clarified the relationship between heart failure and a sleeper’s respiration. Kryger estimates that over the past 40 years, he has treated more than 30,000 people with sleep problems. It’s a gratifying specialty, he says: “We can usually make them better.”
Sleep takes up about a third of our lives. The quality and quantity of sleep we get has a huge impact on our overall health, as individuals and as a nation, with a growing body of research showing that sleep deficits and disorders can contribute to cardiovascular disease, cancer, depression, and other afflictions. And many of those conditions can, on their own, contribute to inadequate sleep. Between 50 and 70 million Americans suffer from sleep disorders; daytime sleepiness costs the economy $18 billion a year in lost productivity and injuries. An estimated 20 percent of car accidents are caused by sleepy drivers, and tiredness has been a factor in many large-scale disasters, including the destruction of the space shuttle Challenger, the Exxon Valdez, and the Chernobyl nuclear plant explosion. For all these reasons, Kryger is always concerned when—as inevitably happens after he delivers a lecture—someone comes up to him and asks, “How do I get my husband to stop snoring?” Snoring can be a sign of sleep apnea. Since Kryger first worked on sleep apnea, the condition has been widely studied. Doctors Vahid Mohsenein and Klar Yaggi at Yale were among the first to demonstrate that it can cause strokes and worsen diabetes. Today 10 percent of the US population—some 30 million people—suffer from it. But there is a highly reliable treatment now: the Continuous Positive Airway Pressure (CPAP) machine, which pumps air to keep the airways open during sleep. It’s not very comfortable at first. The user has to wear a mask over nose and mouth. The sleep center diagnosed David Ortoleva, 68, a retired teacher in New Haven, with sleep apnea and prescribed the CPAP mask. It took him a few months to get used to it. But since he did, “it’s been a life saver.” Another standard treatment, this one for people with insomnia, is cognitive behavioral therapy (CBT). At the sleep center, patients with insomnia may receive individual or group therapy. Lynelle Schneeberg, a clinical psychologist at the center, says patients usually receive two to six sessions, and “it works, people like it, and its effects are lasting.” Schneeberg asks her patients to keep a sleep diary for two weeks. Too often, those with insomnia go to bed earlier than they should, figuring it takes them a long time to fall asleep. But that sleepless interval only reinforces the feeling that one’s bed is a place to be awake in. She reschedules patients’ sleep so that they’ll be in bed only about an hour longer than the number of hours they have been actually sleeping each night; if it’s needed, she adds more time later, in half-hour increments. She also teaches them “stimulus control”: don’t lie awake endlessly; after 20 minutes, sit up and read until you feel drowsy. “You want to distract your brain from all those things it wants to figure out,” she explains. “You’re not thinking about how fabulous your life is at 2 a.m.”—instead, you’re busy “solving all your problems.” Schneeberg often works with patients to reduce the chance that their sleep is interrupted by children, pets, or spouses, or disturbed by too much coffee, alcohol, or cigarettes. She helps them counter their negative beliefs about their ability to get good sleep. Hundreds of randomized controlled studies have shown this course of therapy to be effective. Kathleen Ortoleva, 64—David’s wife and also a retired teacher—swears by it. In her case, she says, “it wasn’t so much not being able to fall asleep, but waking up, waking up, and waking up.” After the sleep center ruled out sleep apnea, Schneeberg took her case. “She made me realize I had to put work into this,” Ortoleva says, “and couldn’t just lie awake every night saying, ‘Well, sleep, where are you?’” Her husband’s sleep issues, which include restless leg syndrome, often interrupted Ortoleva’s own sleep. With Schneeberg’s advice, she decided to put a twin bed in the corner of the bedroom, where she could sleep without disturbance. She started using a mantra every night, praying for people she cared about—and “before you know it, I was sleeping.” Once Schneeberg assured her that getting just five and a half hours or more on most nights was enough to let her function during the daytime, Ortoleva’s recurring 2 a.m. anxiety that she wasn’t getting enough sleep also disappeared, letting her drift back into slumber much more easily. “I became this expert in how to go to sleep,” she says.
Kryger’s most recent book, The Mystery of Sleep, came out last March from Yale University Press. It includes chapters on “Beating Insomnia without Pills” and “Fear of Sleeping and Other Unusual Ailments.” (Ask him about sleep eating or sexomnia, in which a person has sex with their bed partner while asleep.) He is fascinated by the great mysteries of sleep that haven’t yet been unraveled. One of these is “the fact that sleep, or rest, is pervasive throughout nature.” The Nobel Prize for medicine last year went to three scientists whose research was on the genes that control sleep timing. They did this research using fruit flies. Even plants have a circadian rhythm—keeping track of time and, at the right time, going into a kind of sleep. Still more startling, Kryger notes, “bacteria do the same thing. They have periods when they’re very active, and other periods when they’re not active.” Another important puzzle is the relationship of sleep to diseases, including cancer. Every cell in the body has what are called clock genes, which control the timing of the cell’s activity. (The Nobel winners studied clock genes in fruit flies, which share some of those genes with humans.) “Clock genes are synchronized to the main generator of rhythm in the body, which is right in the middle of our brain,” says Kryger. “How does the clock in our brain control all the clocks throughout the body? That is a tremendous mystery.” It’s possible that one reason cancer cells multiply uncontrollably is precisely that they aren’t being controlled: the clock genes may not be functioning. Indeed, some studies of people who have been shift workers for many years have shown that the women are more likely to have breast cancer than other women, and the men more likely to have prostate cancer. Kryger is currently starting research on treatments for people who are extremely sleepy in the daytime, such as narcolepsy sufferers. Because many military veterans with apnea have PTSD and have difficulty using CPAP, he also recently tested oral appliances to treat apnea at the Veterans Affairs hospital in West Haven. This appliance, worn at night, brings the lower jaw up and forward to prevent the apnea; he’s now wrapping up the analysis of the data. Kryger has many colleagues in sleep medicine at Yale. The sleep program, directed by Klar Yaggi, is interdisciplinary, with neurologists, psychologists, pulmonologists, and respiratory specialists involved. Neurologist Brian Koo does research on movement disorders that interfere with sleep. Nancy Redeker at the School of Nursing studies methods of treating sleeplessness in people with chronic diseases without using sleeping pills. Yale’s program is one of a handful nationally that studies and treats the sleep disorders of hospitalized people, with plans for an inpatient sleep testing program at the hospital. The hope is to reduce the number of patients who relapse and have to go back to the hospital, says Christine Won, medical director of the Yale Centers for Sleep Medicine and an associate professor at the Yale School of Medicine. The study of sleep in hospitals grew out of concern for patients with ICU delirium—that is, acute confusion that can emerge during stays in the intensive care unit. ICU delirium coincides with lower chances of survival and more difficult recoveries, says Melissa Knauert, associate program director of Yale’s Sleep Medicine Fellowship. (Kryger is the program director.) One of Knauert’s first research projects at Yale was to put sound meters, light meters, and motion detectors at the doors of ICU rooms to count how many times patients were disturbed. The object was to study the relationship between sleep deprivation and ICU delirium—and the results, says Knauert, were “appalling.” She is now studying circadian rhythms, which contribute to a good night’s sleep, but which can be thrown off by the timing of feeding and other activities in the ICU. “Every organ and cell has a circadian rhythm, and the fact that [hospitals are] ignoring it is compelling,” she says, noting that restorative periods of sleep can be critical for healing. She hopes the study results will help hospitals reduce the number of days of patients’ delirium, the length of their stay, and the level of care they need after being discharged. It’s been difficult to change hospital habits and culture in order to safeguard patient sleep. But Knauert points out that the neonatal intensive care unit is decades ahead—providing hands-off hours when tiny babies are left to sleep without being examined or poked. Hospitals need “a culture change,” she says, so that adult patients can benefit from similar changes that would let them sleep longer and heal more quickly.
What troubles Kryger most is that some people still think sleep is a waste of time, that they’d be better off making money or having fun than lying in bed unconscious. Besides the damage to their own bodies, there can be damage to others. Some of the recent train accidents in the northeastern United States, for instance, were caused by people with sleep apnea. “When someone’s got a disease that can kill other people,” he says, “that’s a public health issue. And it has to be treated.” But also, he values the daily benefits, smaller but still profound, that good sleep produces. One former patient of his (who prefers not to give his name) says that the CPAP treatments he receives even helped his two dogs: “When I [was] down, they seemed to be down,” he says. Now, “they’re just there and peppy.” As for his own health: “When I get up and get going, I feel as if I can get up and get going.”
|

|
 1 comment
1 comment Print
Print Email
Email
1 comment
-

Joseph Lardner, 2:49am March 15 2018 |  Flag as inappropriate
Flag as inappropriate
The comment period has expired.Sleep article.